
It seems everyone is familiar with cortisone. Often recommended early in the treatment of joint, tendon, nerve or bursa related pain, and seen as a ‘quick fix’ by many. A surprisingly high number of the clients we see in the clinic have either undertaken cortisone injection themselves as part of their effort to get pain free, or have been exposed to cortisone injections via a loved one or friend. Have you seen your doctor or other healthcare professional about pain? It’s likely cortisone has come up as a treatment option in your first visit.
Don’t get us wrong, for quick pain relief, cortisone will most likely give you just that. In pain that is severe and acute, absolutely this is a good thing! In conditions that are more chronic however, it’s very likely you won’t feel any better beyond the short term, and there’s a number of well known risks that cortisone injections carry. Cortisone can play a part in a journey to getting pain-free. It is also heavily over-recommended to the general population in conditions where there’s no known benefit in the long term, where exercise and education yield better results, and where the negative consequences haven’t been explained to the patient. Remember, cortisone injections should be a part of your treatment plan, not the only treatment.
This blog aims to tell you what cortisone is, the risks versus the benefits, and when you should consider a cortisone injection as part of your treatment journey.
What is cortisone?
Cortisone is a powerful and commonly prescribed anti-inflammatory for aches and pains of the body. It helps pain by doing exactly what anti-inflammatories do, by reducing the inflammation in the body which in turn can help your pain.
The benefits of cortisone injection
The benefits are plain and simple: in the short term you can likely expect pain relief. How long this lasts is varied and specific to the individual. In long term chronic conditions, expect to feel no better at all.
The risks of cortisone injection
Tendon injuries
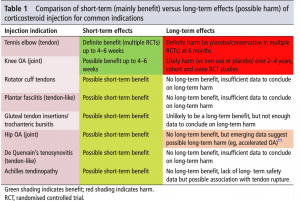
In tendon related conditions (think achilles tendon, tennis elbow pain, gluteal tendinopathy etc.) , cortisone injections have been shown to reduce tendon strength by stopping the formation of connective tissue amongst other things (Kapetanos, 1982). There’s also a possible association with tendon rupture following cortisone injection. (Unverfirth LJ, Olix ML 1973)
In tennis elbow specifically,
“cortisone injections provide short-term pain relief but worsen the condition in the longer term compared with no treatment or placebo treatment.” For clients with tendon injuries we’ve seen in the clinic who’ve undertaken cortisone injections, this seems to be the general consensus.
Osteoarthritis
In osteoarthritis of the hip and knee “the risk of medium-term to long-term complications for both knee and hip OA treated with cortisone injections may be quite high” (Kompel et al. 2019) . In the hip specifically, there’s emerging research that shows the possibility of long term harm including speeding up the rate of osteoarthritis progression. In knee OA and patients awaiting total knee replacement, the research shows that following a cortisone injection, you’ll likely require a total knee replacement earlier than those who haven’t had an injection. Importantly, in research comparing physiotherapy to cortisone injections in knee osteoarthritis they found…
“Significantly less pain and disability in the group who underwent physiotherapy compared to injection” (Deyle et. al 2020)
 (Orchard 2017)
(Orchard 2017)
When should you consider a cortisone injection?
Ultimately, there’s no one size fits all answer to this question. It does depend on the condition, the person’s circumstances, the severity of your pain and the impact your pain is having on your capacity to sleep and function normally. Circumstance is also a big factor for whether cortisone needs to be considered at an earlier date. Take the example of an AFL player with severe foot pain the week of a grand final. A cortisone in this instance is likely to help them firstly reduce their pain in an effort to play as normal. Once the game is completed, treatments aimed at longer term results can be implemented (eg. Physiotherapy)
So in answer to the questions “should I get a cortisone injection?”, here’s our recommendation, based on the research available and our experience in treating thousands of people with lots of different conditions:
As a general rule of thumb, if your pain is acceptable to you and isn’t hugely affecting your day to day life, your sleep isn’t affected and you haven’t yet undertaken 12 weeks of Physiotherapy, don’t look to a cortisone injection for relief. If there are extenuating circumstances, your pain is severe and is heavily impacting your day to day life and you’re sleeping poorly as a result, perhaps a cortisone injection could be helpful in reducing your pain in conjunction with commencing a treatment plan aimed at longer term results. Cortisone is not the fix, but a tool we can use to help manage pain while we address the root cause of your issue.
Conclusion
Unsure if cortisone is something you should consider? Consult an expert Physiotherapist first and get your condition assessed properly. A good physiotherapist will be able to chat through your treatment options, provide you with the risks and benefits of each option, and allow you to make the decision you think is best.
Don’t hesitate to reach out with any questions. Alternatively if you have an ongoing niggle you’d like to get looked at, book a time here, or call the clinic on 8490 0777.
References:
Bisset L, Beller E, Jull G, et al. ‘Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. BMJ 2006;333:939.
Coombes BK, Bisset L, Brooks P, et al. Effect of corticosteroid injection, physiotherapy, or both on clinical outcomes in patients with unilateral lateral Epicondylalgia. JAMA 2013;309:461–9.
Olaussen M, Holmedal Øystein, Mdala I, et al. Corticosteroid or placebo injection combined with deep transverse friction massage, Mills manipulation, stretching and eccentric exercise for acute lateral epicondylitis: a randomised, controlled trial. BMC Musculoskelet Disord 2015;16:122.
Orchard JW, 2020, ‘Corticosteroid injections: glass half full, half empty, or full then empty?’, Br J Sports Med Epub, doi:10.1136/ bjsports-2019-10125