Gluteal tendinopathy is a common injury in athletes who participate in sports that involve a lot of jumping, such as basketball, volleyball, tennis as well as running. It is also common in women over the age of 50 years old, with this study gluteal tendinopathy finding that 1 in 4 in this age group being affected. Common symptoms include swelling and pain around the tendon.
What causes gluteal tendinopathy?
Gluteus medius tendinopathy typically occurs slowly over time due to increased loading and subsequent overloading of the tendon, which can produce pain as the tendon starts to undergo physical changes.
The gluteus medius is one of the three gluteal muscles. It is a fan-shaped muscle that can be found on the side of the hip. The muscle helps move your hip out to the side, as well as rotate the hip outwards.
It also plays a major role in stablising the pelvis during walking and running. The muscle originates from the side of the pelvis and the tendon attaches to the top of the thigh bone.
As a result of this stabilising action, the gluteus medius muscle is the hardest working muscle in the hip when running, absorbing 2.6-3.5 times your body weight.
Gluteus medius tendinopathy is characterised by pain over the outside of the hip (lateral hip). It has traditionally been known as trochanteric bursitis or greater trochanteric pain syndrome, however, advanced imaging and recent evidence as seen in this study which looked at corticosteroid injections vs exercise therapy, has revealed that the primary source of pain is more commonly the gluteus medius tendon with bursal swelling being an accompanying finding.
What are the different stages of gluteal tendinopathy?
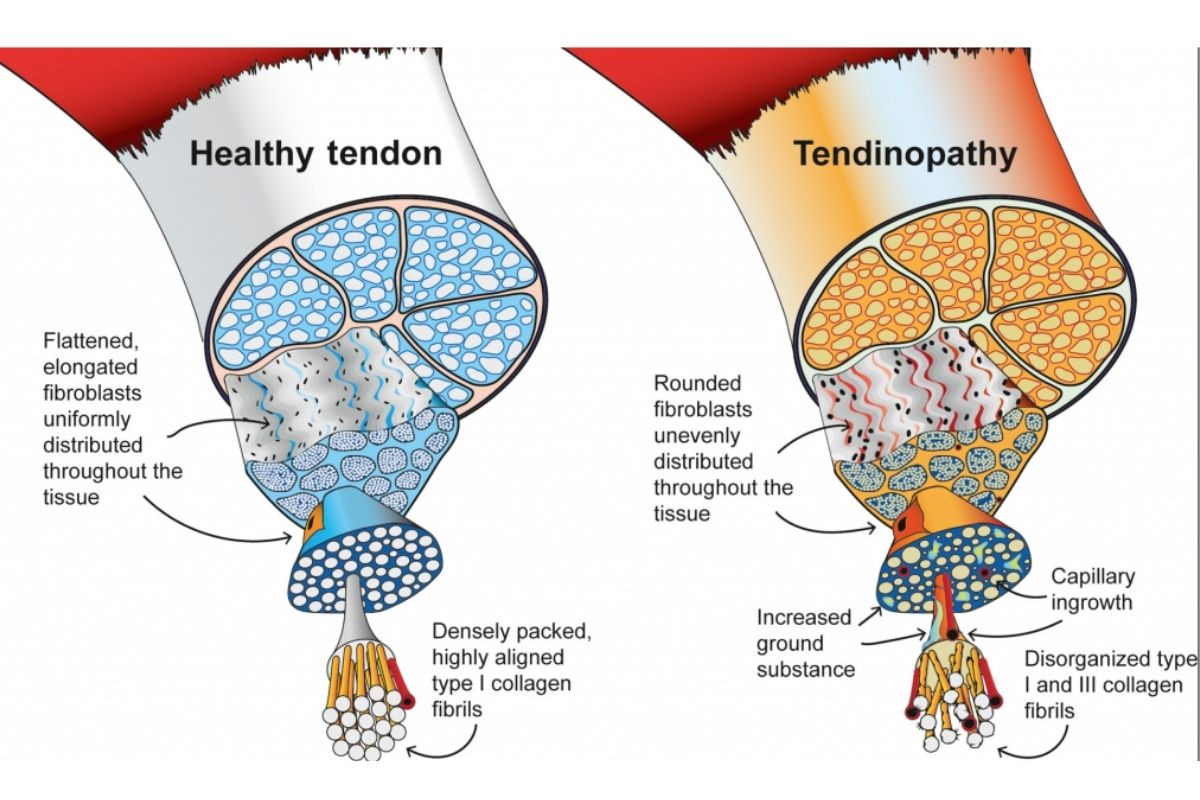
Tendinopathy, including insertional tendinopathies, can be thought to be on a continuum that moves through different phases. Initially, the tendons start to change shape and become thicker, due to chemical and structural changes in the tendon. This is known as the reactive stage.
The tendon thickens in order to reduce the stress and so it can cope with more loading. While the tendon continues to thicken the tendon fibres become disorganised, leaving the tendon with reduced capacity to cope with the force from the muscle contraction. This is known as the disrepair stage.
Over time due to long-term overloading and poor general health, the tendon can move into the degenerative phase, where the death of tendon cells occurs and further disorganisation of the collagen fibres of the tendon. Changes in this phase are irreversible and generally mean the tendon is less tolerant to load. This is known as the degenerative stage.
However, all is not lost, as there are likely portions of the tendon that aren’t in the degenerative phase whose capacity to tolerate load can be improved.
How is gluteal tendinopathy diagnosed?
Gluteal tendinopathy can be diagnosed by a Physiotherapist through a thorough examination including verbal and physical findings. Pain will typically be over the lateral hip and the greater trochanter of the hip where the tendon inserts (this is the large bony bit on the outside of your hip). Pain is typically very localised, with those suffering from it usually reporting an area of pain the width of two fingers. However, pain can also travel down the leg into the thigh and at times as far as the knee.
Morning stiffness is very common, particularly the day after activity. People typically report pain with weight-bearing activities such as walking, standing, running, and climbing stairs.
A common feature of tendon pathologies is what’s called a ‘warm-up pattern’. This means that pain will be present at the start of activity but will ‘warm up’ and reduce throughout the activity. There will sometimes be a threshold during the activity however where the pain may return. Also, the pain may return after activity, as they cool down.
People will also report pain when lying on the sore hip at night, as well as lying on the opposite side. There will also be pain with compression activities such as prolonged sitting, cross leg sitting, and standing with your hip out (also known as ‘lazy standing’).
What are the symptoms of gluteal tendinopathy?
Symptoms of gluteal tendinopathy will include:
- Pain that is localised to the outside of the hip, but can travel down the thigh, but not below the knee
- Pain with contraction of the gluteus medius muscle
- Pain when touching the gluteus medius tendon
- Pain when stretching the gluteus medius muscle
- Pain with standing on one leg
- Pain with stairs
- Pain when lying on your affected side
- Pain with prolonged activity e.g. walking or running
What makes gluteal tendinopathy pain worse?
Below is a table that presents the movement which typically aggravates gluteal tendinopathy pain and how you can avoid them.

Who suffers from gluteal tendinopathy?
Gluteal tendinopathy is more common in females than males. It is the most common tendinopathy in the lower limb and is most likely to affect women between the ages of 40 to 60 years. However, it is also common in the active population, particularly in runners. In the general population, it can also occur in sedentary people due to general deconditioning which leads to weakness and reduced capacity of the tendon to tolerate loads of day-to-day movement.
How long does gluteal tendinopathy take to heal?
Pain that has started over a short period of time, without a long history, is likely in the reactive stage of gluteal tendinopathy. In this case, it can take up from 3-8 weeks to heal as it is likely an acute response to excessive load. During this time, however, complete rest is not the answer. Maintaining some level of activity that is within the load tolerance of the tendon will allow a faster return to your chosen activity.
If the pain has been present for a longer period of time, we’re talking months and years, it may be in the degenerative stage. In this stage, the tendon has likely undergone more structural changes and has become more disorganised. Therefore, patience is required in order to achieve a great result, with tendons in this stage taking 3-6+ months to heal.
Treatments for gluteal tendinopathy
Physiotherapy treatment
Treatment for gluteal tendinopathy varies depending on the severity and the stage the tendinopathy is in.
A progressive strengthening program targeting the lateral hip muscles is where the strongest evidence lies for treating gluteal tendinopathy. This study on the effect of exercises on tissue repair found that strength exercises help promote new tendon fibre growth and therefore help the healing of the tendon.
In the acute stages, some manual therapy provided by a physiotherapist such as soft tissue massage, trigger point release, or dry needling in the gluteal muscles can help reduce pain and improve your confidence and mobility.
A physiotherapist can help prescribe the best exercises for you, depending on your symptoms and what stage your tendinopathy is in, and your current fitness levels. Exercises will start basic and slowly increase in difficulty as pain and function improves. This translates to less pain day-to-day, and greater ease of performing day-to-day activities, and your preferred type of exercise.
An EMG (electromyographic) study from 2011 showed that the best exercise to load your gluteus medius is side-lying leg lifts, followed by single-leg squats and lateral band walks.
Some other exercises that are great for gluteus medius and gluteus maximus strengthening include:
- Single leg deadlift
- Glute bridge
- Sidelying clam
- Forward lunge
- Side lunge
- Forward and side hopping
- Forward and side step ups
Below is a video that features some strengthening exercises commonly used in the rehabilitation of gluteal tendinopathy.
Strength exercise should be completed 2-3 x per week for 8-12 weeks in order to see the greatest benefits. Pain with exercise is okay, but keeping pain at a low level e.g. 4-5/10 should reduce the chance of doing too much too soon and aggravating your condition. Having some lingering pain after an exercise session is ok, so long as your pain returns to baseline within 24 hours.
Education and advice around what is happening in your hip and how to keep active without aggravating your condition are also very important. It is vital to let the tendon have relative rest and avoid aggravation to allow healing in the early stages.
Some load management strategies include:
- Avoiding sitting with legs crossed
- Avoiding lying on painful side
- Placing pillow between knees when lying on unaffected side
- Avoiding stretching glutes
- Avoiding ‘lazy’ standing or hanging on hip
- Reducing walking or running load and avoiding incline if required
Stretching for gluteal tendinopathy
As tendinopathy isn’t a length issue with the tendon and isn’t ‘tight’, stretching is not advised in the treatment of gluteal tendinopathy. In fact, stretching can irritate the already sensitive gluteal tendon, and increase the symptoms associated with gluteal tendinopathy. This is due to the position that is required in order to stretch the gluteal muscles, which involves compressing, therefore irritating, the gluteal tendon.
Cortisone injection for gluteal tendinopathy
Cortisone or corticosteroid injections (a strong anti-inflammatory) can be helpful to reduce pain in the short term when you have completed a minimum of 12 weeks of supervised exercise and have no changes to your symptoms and function. It is important to note that cortisone does not ‘fix the issue, rather it gives the individual some short-term pain relief in order to keep continuing a progressive strengthening program.
Cortisone injections in excess can be detrimental to the health of your tendon, this study on the impact of cortisone injections on tendon health finding that cortisone can have harmful effects on tendon structure as they reduce the tendon strength by reducing healing, stopping the formation of connective tissue.
Shockwave therapy for gluteal tendinopathy
Shockwave therapy has been shown to be effective in treating chronic gluteal tendinopathy. The mechanism of action for shockwave is still unclear, but the current thinking is that it stimulates healing, possibly by stimulating cellular activity and increasing blood flow. A systematic review that looked at the management of greater trochanter pain syndrome (gluteal tendinopathy is included in this) found that those treated maintained benefits for 12 months. It is also recommended that shockwave be used in conjunction with a robust strengthening program.
Surgery for gluteal tendinopathy
Surgery for gluteal tendinopathy can include gluteal tendon repair, removal of the bursa, and removal of the bone underlying the tendon. The proposed mechanism of surgery is to stimulate the tendon environment by improving blood flow and promote healing in the tendon cells. Surgery is generally considered a last resort for long-standing and recalcitrant gluteal tendinopathy, and should only be considered after robust conservative management lasting 12 weeks at the very least.
What next?
For an expert opinion on the next steps for you, or to chat to an expert gluteal tendinopathy physiotherapist, don’t hesitate to reach out by calling the clinic on 8490 0777 or send us an email at [email protected]
If you’re ready to get started on the right path, you can book online using the buttons below.