
An ankle sprain is a very common injury with the majority of these affecting the lateral ligament (outside of the ankle). We look at the evidence for the role of physiotherapy techniques in treating this type of ankle injury.
What is an ankle sprain?
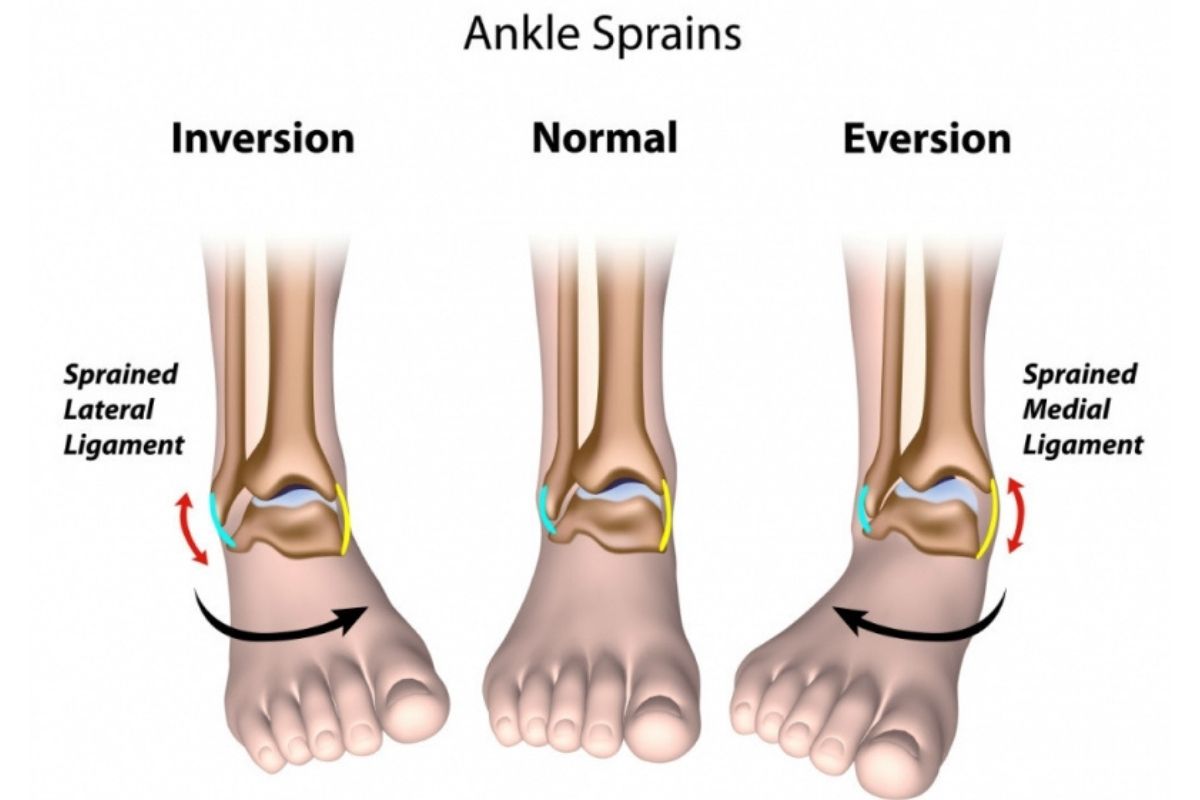
Ankle sprains involve disruption and trauma to the ligaments in the ankle, and mostly occur in the athletic population but do occur in the general population. It is estimated that 10 ankle sprains occur per 1000 exposures and a lateral (inversion) ankle sprain is a four times more common injury than medial (eversion) ankle sprains. An ankle sprain can involve any of the ligaments of the ankle depending on the mechanism of the ankle injury.
How common are ankle sprains?
85% of ankle sprains are of the lateral (outside of your foot) ligaments. These lateral ligaments are made up of the Anterior talofibular (ATFL), Calcaneo-fibular (CTFL), and Posterior talofibular (PTFL).
The ATFL is the most likely ligament to be sprained or injured compared to the CTFL & PTFL due to its anatomical position. This study in 2016 reports the highest incident rate of ankle sprains is largely in sport. In particular, indoor sports carry the highest risk of injury of 7 per 1000 exposures.
A medial ankle sprain is a lot less common and generally involves the large deltoid ligament that stabilizes the medial aspect of the ankle joint. Lastly, high ankle (syndesmosis) sprains involving the anterior inferior tibiofibular ligament (AITF), superficial posterior inferior tibiofibular ligament, transverse tibiofibular ligament, interosseous membrane, interosseous ligament, and the inferior transverse ligament.
Syndesmosis injuries are uncommon ankle injuries, and this study in 2001 reports that 0.5% of all ankle sprains without fracture, and 13% of all ankle fractures involve the syndesmosis. They account for anywhere from 1-11% of all injured ankles. Generally, these types of sprains can be distinguished from a lateral ankle sprain with less swelling, inability to bear weight, and mechanism of injury.
What are the different types of ankle sprains?
Lateral ankle sprains:
They generally involve an inversion action of the ankle joint i.e. rolling onto the outside of your foot (mechanism of injury can also lead to an injured foot as well). There can be immediate pain and generally will swell up quickly with bruising developing later on. A general rule of thumb is the greater the swelling and subsequent bruising, the greater the tissue trauma. Audible pops will sometimes occur, but not always an indication of severity. Generally speaking, weight-bearing will be painful immediately after, and for the first few days. Additionally, you will typically find there is a decrease in range of motion at the ankle joint and swelling.
Medial ankle sprains:
Are an eversion injury of the ankle joint i.e. rolling onto the inside of the foot resulting in an injured ankle. Typically medial ankle sprain occurs when stepping on someone’s foot resulting in the inner ankle ligaments being stressed.
High ankle sprains (syndesmosis injuries):
This type can be caused by forceful amounts of eversion and dorsiflexion that involve the ligaments between the tibia and fibula i.e. the interosseous membrane and ligaments. High ankle and medial sprains are not as common as lateral ligament sprains and are generally more common in a sporting population.
Why you should see a physiotherapist?
Firstly, this study in 2021 found that less than 50% of people seek advice or treatment following lateral ankle sprains, and up to 1/3 of individuals go on to experience chronic ankle instability and recurrent sprains over the next 12 months. Gone are the days of RICE and rest for a few weeks in order to manage an ankle sprain effectively.
Seeing your physiotherapist early can decrease further complications such as persistent pain, stiffness, and ankle strength & proprioception deficits. Our Physiotherapists can assess the degree of severity and instability, assess any function deficits (such as loss of ROM, strength, and proprioception) and rule out anything more serious or sinister injuries such as a fracture.
Ideally, seeing a physiotherapist after 36-48 hours is the best time frame. In the early stages, follow the PEACE & LOVE principles rather than RICE, you can read more about this here. In the acute ankle sprain period, this study in 2013 reports that early physiotherapy is effective in gaining dorsiflexion (ankle ROM) and decreasing pain with manual joint mobilisation. Whilst manual joint therapy has been found beneficial, it should always be used in conjunction with exercise therapy.
This study in 2018 and many others have shown that exercise therapy is effective in reducing recurrent injuries and decreasing the prevalence of ankle instability. Furthermore, supervised exercise can lead to improved ankle strength, proprioception, faster return to sport and work compared to unsupervised exercise.
All in all, effective management of an ankle sprain does not simply include rest, waiting for the pain to subside then returning to activity or sport. A robust rehab program and education are vital to restoring the performance of the ankle joint, the muscles around it as well as reduce the chance of recurrence.
Rehabilitation exercises
In the early stages of ankle rehabilitation, the treatments focus on minimizing swelling, regaining range of motion, and starting some tolerable loading of the ankle joint. Exercise, rehabilitation and treatments will involve strengthening exercises, endurance & power exercises (plyometrics & jumping), and proprioception/balance exercises. For optimal results, the rehabilitation plan should be individualised and formulated after a detailed assessment. It will also depend on the severity of the sprain.
Some exercises include:
Early stage:
- Strengthening exercises for the calf including calf raises (seated or standing) +/- Weight and on / off step
- Ankle eversion & inversion using therabands
- Single leg Balance (proprioception)
- Early landing re-training
- Walking
Mid-late stage:
- Heavier calf raise work (seated or standing) +/- Weight and on / off step
- Jumping & hopping (single & double leg)
- Box jumps & landing skills
- Running (straight line, curve)
- T-test and other agility tests
- Sports/activity specific drills
Below is a video showcasing a few late-stage ankle rehabilitation exercises, including all important strengthening exercises.
Taping techniques
Ankle taping can be used to restrict motion of the ankle in the early stages of rehabilitation to reduce pain, protect the healing process and better allow tolerable loading to the ankle joint. In the sporting population, this study in 2001 found that ankle taping is beneficial to minimise recurrent ankle sprains rather than preventing an initial sprain. These studies in 1984 and 1994 looked at an ankle brace vs no brace in soccer players and found a decrease in recurrent ankle sprains, although there was no difference between the severity of sprain when wearing a brace vs no brace.
Below is an example of a typical taping technique for an ankle sprain:
Recovery time and prognosis
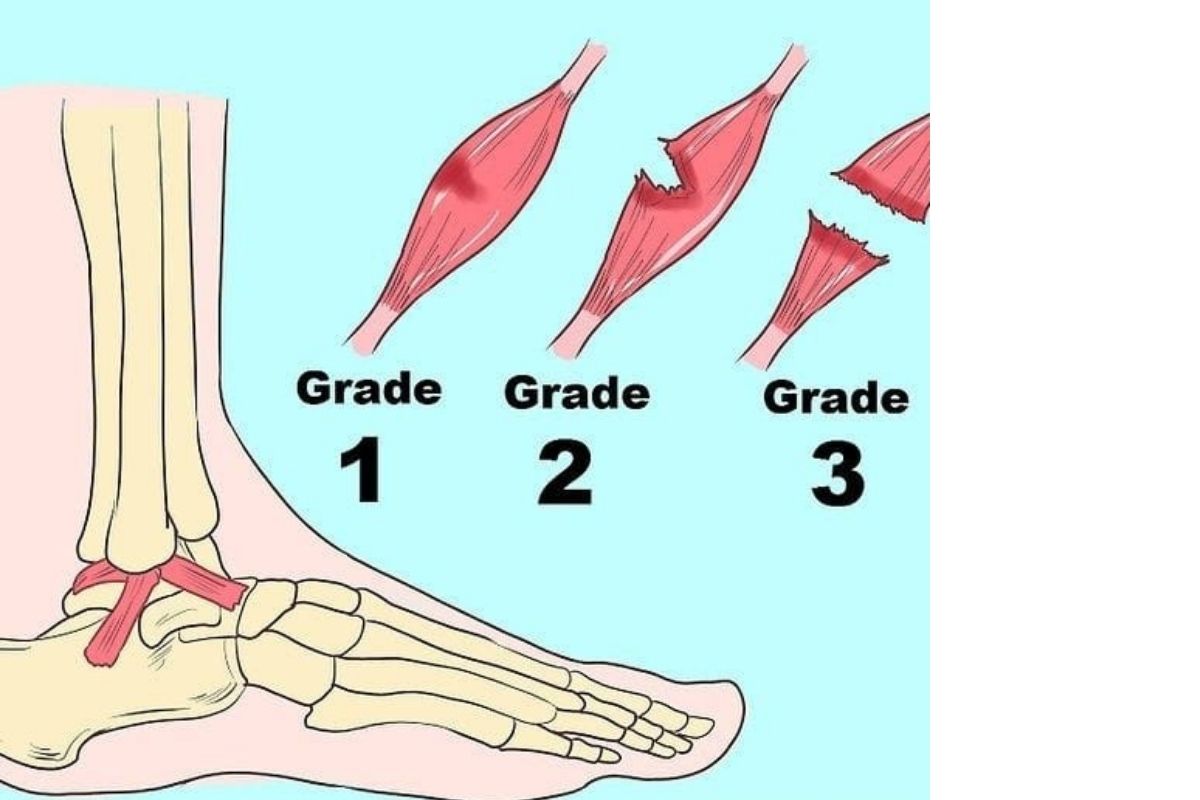
The severity of ankle sprains can be graded into 3 categories, with time frames for return to sport varying for each. The prognosis of an ankle sprain is generally good, with the right rehabilitation.
Grade 1 (Mild) – minimal swelling and tenderness, the little impact of function (2-6 weeks)
Grade 2 (Moderate) – Moderate swelling, pain and is impacting on function i.e. walking and weight-bearing. Reduced ROM and proprioception and perception of instability. (4-8 weeks)
Grade 3 (Severe) – Complete rupture large swelling & pain, loss of function, and increased instability (12 weeks+)
All in all, Physiotherapy provides the most effective and most efficient treatment for ankle sprains. It’s a great way to treat ankle sprains without needing surgery.
Frequently Asked Questions
When can I start walking after an ankle sprain?
We recommend a period of “protecting the injury” for 1 – 2 days, but it is dependent on the grade of injury and the individual. We suggest walking when the pain is tolerable and doesn’t cause any further lingering discomfort lasting longer than 1 hour and returns back to baseline within 24 hours.
Should I wrap a sprained ankle at night?
A compression band can help to combat swelling in your ankle but isn’t required when sleeping at night.
Should I walk on a sprained ankle if it hurts?
Yes, pain does not equal tissue damage, so beginning to walk on your ankle after a sprain as early as your pain allows can kick start your recovery.
What next?
If you’d like to chat with one of our expert physios, please don’t hesitate to call us on 8490 0777 or email us at [email protected]
If you’re ready to start your ankle sprain rehabilitation or are interested in a tailored injury prevention program, you can book online for a Physiotherapy appointment here.
We look forward to hearing from you!